Cancer of the Larynx & Voice Box
The larynx is an organ at the front of your neck. It is also called the voice box. It is about 2 inches long and 2 inches wide. It is above  the windpipe (trachea). Below and behind the larynx is the esophagus. the windpipe (trachea). Below and behind the larynx is the esophagus.
The larynx has two bands of muscle that form the vocal cords. The cartilage at the front of the larynx is sometimes called the Adam’s apple.
The larynx has three main parts:
- The top part of the larynx is the supraglottis.
- The glottis is in the middle. Your vocal cords are in the glottis.
- The subglottis is at the bottom. The subglottis connects to the windpipe.
The larynx plays a role in breathing, swallowing, and talking. The larynx acts like a valve over the windpipe. The valve opens and closes to allow breathing, swallowing, and speaking:
- Breathing: When you breathe, the vocal cords relax and open. When you hold your breath, the vocal cords shut tightly.
- Swallowing: The larynx protects the windpipe. When you swallow, a flap called the epiglottis covers the opening of your larynx to keep food out of your lungs. The food passes through the esophagus on its way from your mouth to your stomach.
- Talking: The larynx produces the sound of your voice. When you talk, your vocal cords tighten and move closer together. Air from your lungs is forced between them and makes them vibrate. This makes the sound of your voice. Your tongue, lips, and teeth form this sound into words.
Who’s at Risk?
 |
No one knows the exact causes of cancer of the larynx. Doctors cannot explain why one person gets this disease and another does not. We do know that cancer is not contagious. You cannot “catch” cancer from another person.
People with certain risk factors are more likely to get cancer of the larynx. A risk factor is anything that increases your chance of developing this disease.
Studies have found the following risk factors: |
- Age. Cancer of the larynx occurs most often in people over the age of 55.
- Gender. Men are four times more likely than women to get cancer of the larynx.
- Race. African Americans are more likely than whites to be diagnosed with cancer of the larynx.
- Smoking. Smokers are far more likely than nonsmokers to get cancer of the larynx. The risk is even higher for smokers who drink alcohol heavily.
People who stop smoking can greatly decrease their risk of cancer of the larynx, as well as cancer of the lung, mouth, pancreas, bladder, and esophagus. Also, quitting smoking reduces the chance that someone with cancer of the larynx will get a second cancer in the head and neck region. (Cancer of the larynx is part of a group of cancers called head and neck cancers.)
- Alcohol. People who drink alcohol are more likely to develop laryngeal cancer than people who don’t drink. The risk increases with the amount of alcohol that is consumed. The risk also increases if the person drinks alcohol and also smokes tobacco.
- A personal history of head and neck cancer. Almost one in four people who have had head and neck cancer will develop a second primary head and neck cancer.
- Occupation. Workers exposed to sulfuric acid mist or nickel have an increased risk of laryngeal cancer. Also, working with asbestos can increase the risk of this disease. Asbestos workers should follow work and safety rules to avoid inhaling asbestos fibers.
Other studies suggest that having certain viruses or a diet low in vitamin A may increase the chance of getting cancer of the larynx. Another risk factor is having gastroesophageal reflux disease (GERD), which causes stomach acid to flow up into the esophagus.
Most people who have these risk factors do not get cancer of the larynx. If you are concerned about your chance of getting cancer of the larynx, you should discuss this concern with your health care provider. Your health care provider may suggest ways to reduce your risk and can plan an appropriate schedule for checkups.
Symptoms
The symptoms of cancer of the larynx depend mainly on the size of the tumor and where it is in the larynx. Symptoms may include the following:
- Hoarseness or other voice changes
- A lump in the neck
- A sore throat or feeling that something is stuck in your throat
- A cough that does not go away
- Problems breathing
- Bad breath
- An earache
- Weight loss
These symptoms may be caused by cancer or by other, less serious problems. Only a doctor can tell for sure.
Diagnosis
If you have symptoms of cancer of the larynx, the doctor may do some or all of the following exams:
- Physical exam. The doctor will feel your neck and check your thyroid, larynx, and lymph nodes for abnormal lumps or swelling. To see your throat, the doctor may press down on your tongue.
- Indirect laryngoscopy. The doctor looks down your throat using a small, long-handled mirror to check for abnormal areas and to see if your vocal cords move as they should. This test does not hurt. The doctor may spray a local anesthesia in your throat to keep you from gagging. This exam is done in the doctor's office.
- Direct laryngoscopy. The doctor inserts a thin, lighted tube called a laryngoscope through your nose or mouth. As the tube goes down your throat, the doctor can look at areas that cannot be seen with a mirror. A local anesthetic eases discomfort and prevents gagging. You may also receive a mild sedative to help you relax. Sometimes the doctor uses general
 anesthesia to put a person to sleep. This exam may be done in a doctor's office, an outpatient clinic, or a hospital. anesthesia to put a person to sleep. This exam may be done in a doctor's office, an outpatient clinic, or a hospital.
- CT scan. An x-ray machine linked to a computer takes a series of detailed pictures of the neck area. You may receive an injection of a special dye so your larynx shows up clearly in the pictures. From the CT scan, the doctor may see tumors in your larynx or elsewhere in your neck.
- Biopsy. If an exam shows an abnormal area, the doctor may remove a small sample of tissue. Removing tissue to look for cancer cells is called a biopsy. For a biopsy, you receive local or general anesthesia, and the doctor removes tissue samples through a laryngoscope. A pathologist then looks at the tissue under a microscope to check for cancer cells. A biopsy is the only sure way to know if a tumor is cancerous.
If you need a biopsy, you may want to ask the doctor the following questions:
- What kind of biopsy will I have? Why?
- How long will it take? Will I be awake? Will it hurt?
- How soon will I know the results?
- Are there any risks? What are the chances of infection or bleeding after the biopsy?
- If I do have cancer, who will talk with me about treatment? When?
Staging
To plan the best treatment, your doctor needs to know the stage, or extent, of your disease. Staging is a careful attempt to learn whether the cancer has spread and, if so, to what parts of the body. The doctor may use x-rays, CT scans, or magnetic resonance imaging to find out whether the cancer has spread to lymph nodes, other areas in your neck, or distant sites.
Treatment
People with cancer of the larynx often want to take an active part in making decisions about their medical care. It is natural to want to learn all you can about your disease and treatment choices. However, shock and stress after a diagnosis of cancer can make it hard to remember what you want to ask the doctor. Here are some ideas that might help:
- Make a list of questions.
- Take notes at the appointment.
- Ask the doctor if you may use a tape recorder during the appointment.
- Ask a family member or friend to come to the appointment with you.
Your doctor may refer you to a specialist who treats cancer of the larynx, such as a surgeon, otolaryngologist (an ear, nose, and throat doctor), radiation oncologist, or medical oncologist. You can also ask your doctor for a referral. Treatment usually begins within a few weeks of the diagnosis. Usually, there is time to talk to your doctor about treatment choices, get a second opinion, and learn more about the disease before making a treatment decision.
Methods of Treatment
Cancer of the larynx may be treated with radiation therapy, surgery, or chemotherapy. Some patients have a combination of therapies.
Radiation therapy (also called radiotherapy) uses high-energy x-rays to kill cancer cells. The rays are aimed at the tumor and the tissue around it. Radiation therapy is local therapy. It affects cells only in the treated area. Treatments are usually given 5 days a week for 5 to 8 weeks.
Laryngeal cancer may be treated with radiation therapy alone or in combination with surgery or chemotherapy:
- Radiation therapy alone: Radiation therapy is used alone for small tumors or for patients who cannot have surgery.
- Radiation therapy combined with surgery: Radiation therapy may be used to shrink a large tumor before surgery or to destroy cancer cells that may remain in the area after surgery. If a tumor grows back after surgery, it is often treated with radiation.
- Radiation therapy combined with chemotherapy: Radiation therapy may be used before, during, or after chemotherapy.
After radiation therapy, some people need feeding tubes placed into the abdomen. The feeding tube is usually temporary.
These are questions you may want to ask your doctor before having radiation therapy:
 |
- Why do I need this treatment?
- What are the risks and side effects of this treatment?
- Are there any long-term effects?
- Should I see my dentist before I start treatment?
- When will the treatments begin? When will they end?
- How will I feel during therapy?
- What can I do to take care of myself during therapy?
- Can I continue my normal activities?
- How will my neck look afterward?
- What is the chance that the tumor will come back?
- How often will I need checkups?
|
Surgery is an operation in which a doctor removes the cancer using a scalpel or laser while the patient is asleep. When patients need surgery, the type of operation depends mainly on the size and exact location of the tumor.
There are several types of laryngectomy (surgery to remove part or all of the larynx):
- Total laryngectomy: The surgeon removes the entire larynx.
- Partial laryngectomy (hemilaryngectomy): The surgeon removes part of the larynx.
- Supraglottic laryngectomy: The surgeon takes out the supraglottis, the top part of the larynx.
- Cordectomy: The surgeon removes one or both vocal cords.
Sometimes the surgeon also removes the lymph nodes in the neck. This is called lymph node dissection. The surgeon also may remove the thyroid.
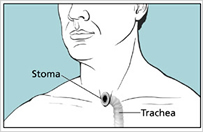
During surgery for cancer of the larynx, the surgeon may need to make a stoma. (This surgery is called a tracheostomy.) The stoma is a new airway through an opening in the front of the neck. Air enters and leaves the windpipe (trachea) and lungs through this opening. A tracheostomy tube, also called a trach (“trake”) tube, keeps the new airway open. For many patients, the stoma is temporary. It is needed only until the patient recovers from surgery. More information about stomas can be found in the “Living with a Stoma” section.
After surgery, some people may need a temporary feeding tube.
Chemotherapy is the use of drugs to kill cancer cells. Your doctor may suggest one drug or a combination of drugs. The drugs for cancer of the larynx are usually given by injection into the bloodstream. The drugs enter the bloodstream and travel throughout the body.
Chemotherapy is used to treat laryngeal cancer in several ways:
- Before surgery or radiation therapy: In some cases, drugs are given to try to shrink a large tumor before surgery or radiation therapy.
- After surgery or radiation therapy: Chemotherapy may be used after surgery or radiation therapy to kill any cancer cells that may be left. It also may be used for cancers that have spread.
- Instead of surgery: Chemotherapy may be used with radiation therapy instead of surgery. The larynx is not removed and the voice is spared.
Chemotherapy may be given in an outpatient part of the hospital, at the doctor’s office, or at home. Rarely, a hospital stay may be needed.
These are questions you may want to ask your doctor before having chemotherapy:
- Why do I need this treatment?
- What will it do?
- Will I have side effects? What can I do about them?
- How long will I be on this treatment?
- How often will I need checkups?
>> Back to Larynx & Voicbox Conditions
|

